

Another Inexplicable Brick In the Wall
Leave Those Kids Alone

On Monday the Health Secretary here in the UK announced - following advice from the Joint Committee on Vaccination and Immunisation (JCVI) - that "[healthy] children aged between 12 and 15 should be given a second dose 12 weeks from the first dose". This underlying advice has not yet been made publicly available, but apparently the JCVI “felt that accelerating the programme would maximise protection for individuals”. Hmm. Surely a “feeling” is not enough to justify such a decision, especially as the JCVI only a few months ago couldn’t get comfortable advising a first dose for this age group, and specifically noted a higher risk of serious adverse effects after the second dose?
I worry that evidence-based medicine has given way to pharmaceutical politicking.
The Vaccine Saviour Narrative: A False Prophesy
I have previously written about the various decisions made by the authorities to give children Covid-19 vaccines, and I have consistently argued that this is a complete madness. The logic is perverse.
On 8 December 2020, shortly after the various Covid vaccine trial results had been published, I wrote the following:
It is a false prophecy to infer that this vaccine will stop the spread of disease that is caused by an endemic virus to which the population is known to (now) have a high degree of inherent resistance.
This statement is not only correct, it is also surprising that anyone should have thought – at the time – that it might not be. Let alone now, almost a year later.
The ‘Vaccine Saviour’ narrative is flawed, and the above statement was not a difficult prediction to make based on how the trials were constructed. It further calls into question the competence of those who called for harmful restrictions – lockdowns, masks and the like – in January 2021 as the ‘vaccine cavalry is just around the corner’.
I have generally in my life been pretty pro vaccination under the “vaccines cause adulthood” principle. Perhaps I was naive in thinking this. But for all the past mistakes, and noting that all medical interventions have potential side effects, vaccinating children against extremely dangerous diseases that both stops them getting it AND passing it on (= sterilising immunity) seems unarguable. When our youngest daughter was only a few hours old we ignored a midwife who was attempting to put us off giving consent for her to receive a TB vaccine: “she might have a big mark on her arm”, we were told. I thanked her for her views and we signed the consent form.
But no medical intervention is without risk, and that is where we have to move away from binary “vaccine good / bad” distinctions. I have discussed the ideas of asymmetric risk profiles on numerous occasions over the last year or so: what is good for the goose might not be good for the gander. Moreover (and appropriately extending the bird-related metaphor) things that are bad for the goose might also be extremely bad for the gander. For example, since the introduction of leaky vaccines, Marek’s disease — an illness of fowl — has become fouler:
The Marek’s vaccine is “imperfect” or “leaky.” That is, it protects chickens from developing disease, but doesn’t stop them from becoming infected or from spreading the virus. Inadvertently, this made it easier for the most virulent strains to survive. Such strains would normally kill their hosts so quickly that they’d die out. But in an immunised flock, they can persist because their lethal nature has been neutered.
This is a trade-off that you might accept if the vaccine was seriously making a difference in reducing all-cause mortality, which unfortunately is not the case. The concept of vaccine escape – and the long-term evolution of SARS-CoV-2 – is discussed in this government document published in the summer. There is a whole lot more to explore in this area, and I covered the implications of some of these thought processes earlier in the year: “there is no point invoking the precautionary principle to encourage across-the-board vaccination now if there is even a sliver of doubt about the possibility of an “own goal” ADE-enhanced epidemic next winter”.
This is consistent with how the vaccine programme was sold to a credulous populace in the latter part of 2020. Thus spake the Vaccine Tsar, Kate Bingham, at the time:
“People keep talking about ‘time to vaccinate the whole population’, but that is misguided,” she said. “There’s going to be no vaccination of people under 18. It’s an adult-only vaccine, for people over 50, focusing on health workers and care home workers and the vulnerable”.
Quite so. While it was entirely rational to offer a vaccine for those at risk, attempts to ram a needle into every arm in the country (1) was never part of the plan (or so we were told…), (2) was never going to provide material benefit to younger age groups and (3) could potentially cause a great deal of immediate harm from unnecessary adverse effects, as well as (4) creating substantial potential long-term bad happenings.
The idea of vaccinating children is therefore especially egregious, as it brings into play the possibility that one might be foisting a medical procedure on a child that they do not need, and might well result in net harms. Children should not be human shields for adults.
The key point is that the risk of a severe ‘life-changing or life-ending’ outcome from Covid for these age groups is essentially negligible. For example, a recent pre-print points out that in Germany (with 13.7 million under the age of 18) :“among children with no comorbidities… no deaths [were] reported in children ≥ 5 years of age” up to and including May 2021.
No Attempt To Justify The Unjustifiable
So how can it be that on Monday the JCVI advised that "[healthy] children aged between 12 and 15 should be given a second dose 12 weeks from the first dose", and moments later the Health Secretary enthusiastically embraces this recommendation? This decision plumbs new lows. At least they had the decency back in September to run a few press conferences in a hollow caricature of due process.
Back then, the JCVI did not advise proceeding with the first dose for that age group: "Available data from the US and Canada indicate the reporting rate of myocarditis is higher following a second dose of mRNA vaccine, compared with the first dose" and "the clinical picture is atypical and the medium to long-term (months to years) prognosis, including the possibility of persistence of tissue damage resulting from inflammation, is currently uncertain as sufficient follow-up time has not yet occurred":
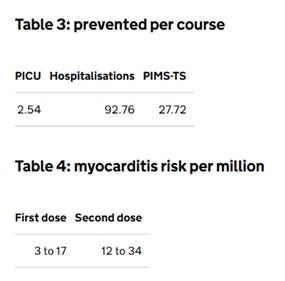
This first dose estimate of myocarditis rates is repeated in another paper released by UKHSA (the UK Health and Security Agency) this week entitled Myocarditis and pericarditis after COVID-19 vaccination: guidance for healthcare professionals: "As of 17 November 2021, the overall reporting rate across all age groups for myocarditis following vaccination with the Pfizer vaccine is 10 per million doses".
But we also know that this is skewed towards younger people. So if the average is 10 per million doses... well, you don't need me to do the maths.
And even 3-17 cases of myocarditis per million doses was not enough to justify the injection for this age group back in September.
The rest of the document is a shocking read:
“most patients who develop symptoms have usually been vaccinated with a mRNA vaccine (Pfizer or Moderna)"… "myocarditis – significant left ventricular (LV) fibrosis has been described in a high percentage of children admitted to hospital... with a small percentage of these having non-sustained ventricular tachycardia (VT)… no follow-up data is available yet on hospitalised patients".
No follow-up data?!?!? Myocarditis is for life – heart function can be permanently impaired.
From the table above, the second dose raises the myocarditis risk from 10 per million to 12 to 34 per million, i.e. potentially more than 3x the risk from this adverse effect alone.
For what gain? A recent article in The Lancet notes that "it appears to be grossly negligent to ignore the vaccinated population as a possible and relevant source of transmission when deciding about public health control measures".
It is even more disturbing if we go back to the decision by the Chief Medical Officers to over-rule the JCVI and proceed with the first dose for 12-15 year-olds. The JCVI stated at the time: "Delivery of a COVID-19 vaccine programme for children and young people is likely to be disruptive to education in the short term, particularly if school premises are used for vaccination" and “Adverse reactions to vaccination (such as fevers) may also lead to time away from education for some individuals".
But now, the JCVI somehow see fit to go ahead with the second jab for 12-15 year-olds, despite other places, such as Taiwan, suspending the Pfizer second dose for all children. Are children in Taiwan genetically different from British kids?
You will be pleased to hear that Pfizer are looking into this. Research "to characterize the clinical course, risk factors, long-term sequelae, and quality of life in children and young adults <21 years with acute post-vaccine myocarditis" is underway.
The bad news? It will report in 2025:
It strikes me that we should be waiting to see these results before potentially harming our children.
Monday’s decision by the JCVI is nothing but extraordinarily odd. It will cost a huge amount of money (including an increase in the premium per shot delivery by each GP – how is this ethical?), could fuel vaccine escape, has the potential for causing life-changing harm (or worse) and will disrupt children’s education. Again: for what?
Children have been mercifully unaffected by Covid, and caution is the better part of valour: it cannot be ethical to push a vaccine on them that could cause serious – and as yet unknown – long-term harm.
In the meantime, we should follow expert advice:
Circulation of SARS-CoV-2 may in fact be desirable, as it is likely to lead to primary infection early in life when disease is mild, followed by booster re-exposures throughout adulthood as transmission blocking immunity wanes but disease blocking immunity remains high. This would keep reinfections mild and immunity up to date.
Let's leave these kids alone.
Subscribe to Alex Starling's Substack
Challenging the Narrative